
Scale of Failure
A practical way to talk about failure without blame, so we can learn faster and build quality in.

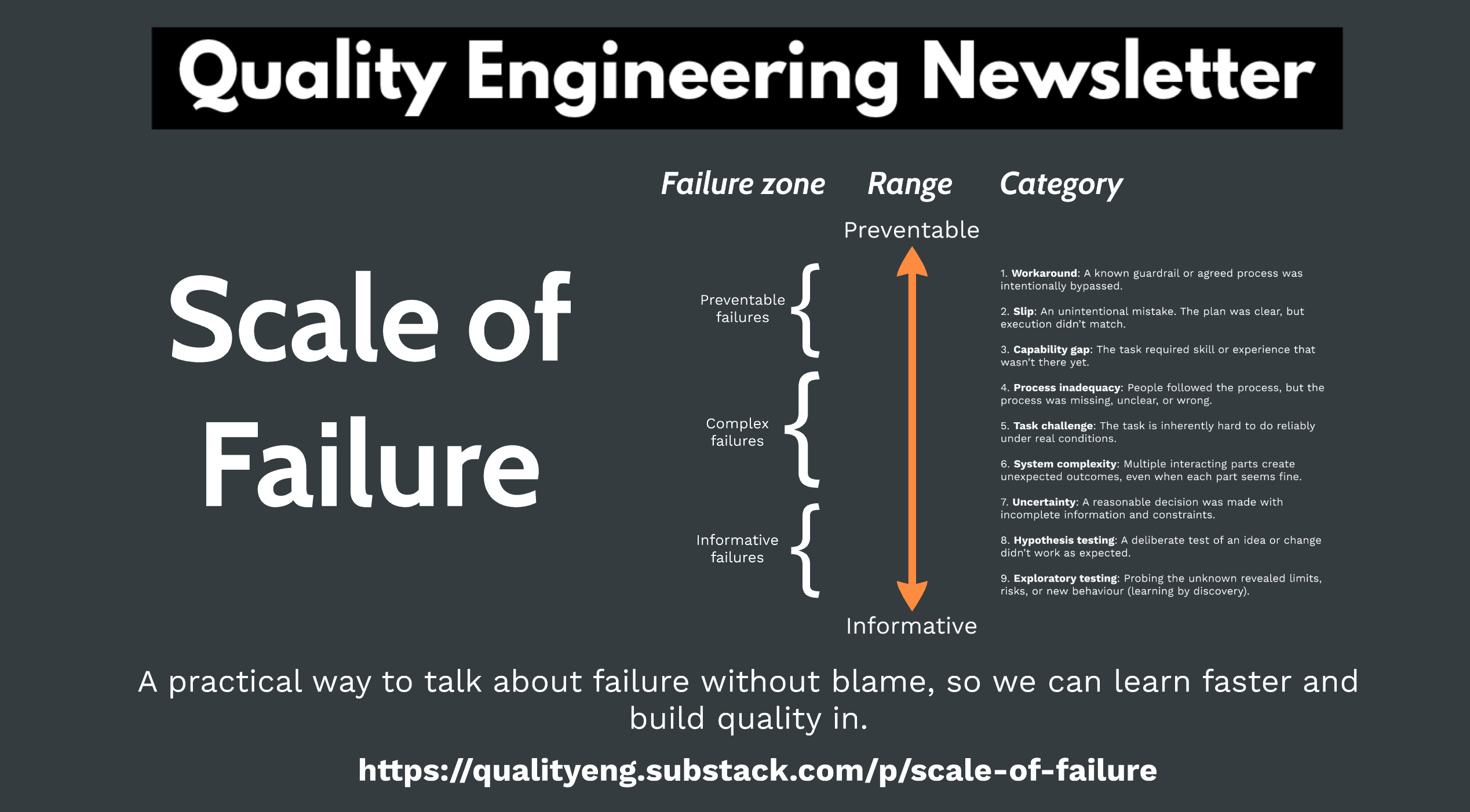
We tend to treat all failures the same. This pushes teams into one of two defaults: root cause analysis for everything, or a quick patch and move on. This scale helps you pick a response that improves the system, not just the symptom.
Spectrum of reasons for why failure occurs
How? Well, this is where we can borrow some ideas from Amy Edmondson’s 2011 HBR post Strategies for Learning from Failure. In this post, Amy shared a spectrum of reasons why failure occurs.
Her spectrum places failure on a range from praiseworthy to blameworthy. Praiseworthy failures are all about learning, while blameworthy failures often feel deliberate. Everything in between tends to be accidents, mistakes, or chance.
Note: Amy wasn’t saying we should literally blame people for failure. It was more about how people tend to feel about the reasons for failure in that range.
Keep reading with a 7-day free trial
Subscribe to Quality Engineering Newsletter to keep reading this post and get 7 days of free access to the full post archives.